Introduction
Dear parents! Here is a guide to preparing children from birth to two years of age for prosthetics. But before telling you about its contents, and even before introducing its author, we congratulate you on a very important event – the appearance of a new person in your family! This is incredible joy, a huge celebration and a miracle that should be felt and experienced right here and now. A happy, confident and calm parent is much more important for a child than any prostheses, rehabilitation and physiotherapy procedures.
We are also parents, some members of our team also have children with special needs. So we understand the range of emotions you may experiencing now. Accepting your child's uniqueness and overcoming fears about the future can be quite challenging. But when there is a clear plan and clear information about the opportunities, goals and methods for achieving them, it becomes easier. That's why we are here to give you this information.
There are not many reasons for concern from a medical point of view regarding the “special” hand. The vast majority of our “children” develop on par with their peers, and in some ways even surpass them. They are completely independent, go to the most ordinary kindergartens and schools, ride bicycles and scooters, play sports, win medals, draw, climb trees, act in plays, play pranks, in general, they live a real child’s life. Adult users of our devices find work in completely different industries such as traveling, running fashion blogs, building houses, planting trees and having children. In general, in our experience (and we have more than 2000 prosthetics over our shoulders), happiness and success in life depend little on whether your hands look alike.
Now let's get acquainted with the main author of our manual. Alina Kuzyakina is a medical rehabilitation doctor, pediatrician, Master of Healthcare Management, and mother of two boys. She studied in Russia and Canada, attended many international conferences, and gave presentations on prosthetics and rehabilitation for children.
One of the main ideas of our doctor is to use this material to give you an understanding that you are not alone, and there are people nearby who will be happy to help you. Therefore, if during the process of reading material you or family members have questions or thoughts that you would like to share, you can contact Alina by phone and email listed at the end of the manual.
Enjoy reading, let it be useful!

First contact with world of modern prosthetic technologies
So, your family has a baby with a special upper limb. We regard this not as a disease, but rather as a developmental feature. This is important both for understanding the wording in this manual and for internal awareness. Your child is not sick, the kid is healthy! He just has this peculiarity of his upper limb. And we are sure that the kid has other unique traits, they may well be particularly smart or kind, or perhaps your kid has incredible drawing skills or is a natural actor of large and small stages. These are all characteristics that we live with and that make us who we are.
We don't know why one hand is different from the other. Doctors and scientists identify various factors, but most of our parents were never exposed to them. You can devote several pages to research and years to self-analysis, but there is no need for this. This does not change reality, and there is no reason to change it, here is a beautiful and healthy child.
This beautiful and healthy child has their own needs. The need for care and love are the most important. Another, quite significant, need is for an upper limb prosthesis. Here a certain dissonance arises, we treat the child as if the kid is healthy. But how then can we fit the need for technical means of rehabilitation into this concept? This is very simple. Let's figure out why our children need prostheses and whether it is possible to do without them.
Some of NOT boring numbers
It is possible to live without prosthetics! Not long ago, we conducted a survey of 100 families immediately before the installation of the first prosthesis for their children. And we found that 93% of our patients are completely adapted to everyday life, they do not experience difficulties with any activities and do not require “additional” help. The remaining 7% had minimal difficulties, for example, with laces and zippers. Children were a little slower to master them, or families simply avoided these clothing items, for example by replacing laces with hook & loop.

Do we really need a prosthesis?
If a child can be completely independent without a prosthesis, why is a prosthesis needed? There are several important points.
The prosthesis helps the back muscles to develop correctly. Without a prosthesis, one arm works more than the other. Also, the marked differences in weight between two sides of the body cannot be overlooked. These factors influence the formation of posture. Back posture does matter. A straight back is beautiful. But what is much more significant is that when posture is changed, sooner or later discomfort and pain arise. It will be difficult for a kid to sit at a school desk or carry a school bag, and there will be limitations in active movement or playing sports. Once scoliosis has already formed, it is extremely difficult to “unbend” the spine and correct everything. This is why it is important to avoid this situation or to prevent its further development if disorders already exist. This is why prosthesis is needed. Let's not forget about the arm muscles that require prosthetics, a prosthesis allows to increase muscle strength, then in the shoulder area one arm will not look thinner than the other.
Surprisingly, the peculiarity of one arm causes changes in the other limb over time. When you refuse to use a prosthesis, all the load falls on the second arm. Because of this, its joints, ligaments and fascia become overloaded. In foreign literature, this is called overuse syndrome — a conditionally “healthy” arm begins to hurt and requires close medical monitoring, and, most likely, treatment.
A prosthesis is uncommon and stylish. Perhaps, this is not the strongest motivation for you and your kid right now, but over time it may come to the fore. Walking without a prosthesis is also normal. The hand is different, but that doesn't make it ugly. We do not mean the absolute necessity of a prosthesis for “disguise”, but that the device can be used as a kind of accessory.
Prosthetics is currently developing at a tremendous pace, new technologies and devices are constantly emerging, bank cards and fitbits are already being built into adult and teenage prostheses. Several laboratories around the world are working on enabling a person to feel objects and touch with a prosthesis. However, to be able to use the coolest developments of the future, it is important to wear and be able to use the prostheses of the present. Otherwise, the muscles may not be ready for installation of another type of prosthesis (bionic), and the prosthesis cannot be used.
So, today a prosthesis cannot completely replace a hand, while progress towards this begins. But along this way it is very important to take from modern technologies what they can give here and now. A prosthesis is not a replacement for a hand, it is the child’s overall health and the opportunity to choose in the future. Perhaps this is the main idea of this chapter.
How to get a prosthesis?
The system of providing technical means of rehabilitation works differently in different countries. At the time of writing this guide, every citizen in Russia whose individual rehabilitation and habilitation program includes a prosthesis has the right to receive it free of charge. The full text of the rules for providing disabled people with technical means of rehabilitation is described in the RF Government Resolution dated 07.04.2008 No. 240 “On the procedure for providing disabled people with technical means of rehabilitation and certain categories of citizens from among veterans with prostheses (except dental), prosthetic and orthopedic products.” Here we will try to give a simplified and understandable algorithm of actions for getting a prosthesis.
Step 1
Contact a prosthetic company seeking advice. This can be done even at a very young age to understand what options are available and when to take the next step. Motoriсa team provides both in-person and remote consultations.
Step 2
After consultation with the prosthetic company, you need to draw up an individual rehabilitation and habilitation program for the disabled person (IRHP). Our kids are considered disabled. And, frankly speaking, this also sets our teeth on edge. But this is a formality that allows you to get a prosthesis for free. To draw up an IRHP, you should visit a number of doctors at the clinic and pay a special commission. At all these stages, we will definitely help you if necessary.
Step 3
Once the prosthesis is registered in IRHP, a decision can be made on the prosthesis acquisition scheme. Motorica offers different options so that each family can choose the most convenient scheme for themselves:
Payment with own funds with subsequent compensation from the Social Insurance Fund (SIF). The easiest and fastest option is to buy a prosthesis and wait for money to be returned to you by the government.
Obtaining non-interest-bearing loans from a partner bank, the loan can be repaid after receiving compensation for prosthetics from the government.
Receiving a prosthesis for free through a government tender. The implementation period is up to six months, there are some pitfalls here, but the purchase is immediately made at state expense.
Contacting a charity for help. Our foundation has already helped many children. People who participate in the purchase of a prosthesis do it with all their heart and are very happy when they manage to do an important and good deed.
If you are unable to obtain an IRHP or you do not wish to collect documents and attend commissions, you can purchase a prosthesis at your own expense. It should be noted separately that the maximum compensation for the cost of a prosthesis may differ in different regions. In some regions the government pays the full cost of the device, and in others parents have to pay part of the funds themselves, and in such a situation the help of a charitable foundation can be very useful.
Payment with own funds with subsequent compensation from the Social Insurance Fund (SIF). The easiest and fastest option is to buy a prosthesis and wait for money to be returned to you by the government.
Obtaining non-interest-bearing loans from a partner bank, the loan can be repaid after receiving compensation for prosthetics from the government.
Receiving a prosthesis for free through a government tender. The implementation period is up to six months, there are some pitfalls here, but the purchase is immediately made at state expense.
Contacting a charity for help. Our foundation has already helped many children. People who participate in the purchase of a prosthesis do it with all their heart and are very happy when they manage to do an important and good deed.
If you are unable to obtain an IRHP or you do not wish to collect documents and attend commissions, you can purchase a prosthesis at your own expense. It should be noted separately that the maximum compensation for the cost of a prosthesis may differ in different regions. In some regions the government pays the full cost of the device, and in others parents have to pay part of the funds themselves, and in such a situation the help of a charitable foundation can be very useful.
Step 4
Get a prosthesis. We provide prosthetics in Moscow and in 85 regions of Russia. In any case, the prosthesis is delivered from our Moscow laboratory for prosthetics. It is made in advance based on measurements, photographs and videos that you send via email. Based on this data, engineers design the prosthesis on a computer, print it on a 3D printer, paint, dry and test it. At the time of prosthetics, a prosthetic socket is made on site, a special glove that is placed between hand and prosthesis. The prosthetist “sculpts” it onto the child’s limb. It should fit as tightly as possible to the stump - not slip or move, but at the same time not squeeze the hand too much. Once the socket is ready, it is attached to the prosthesis, resulting in a fully-fledged device that can be used to pick up and release objects.

What types of prostheses are there?
It is likely that you have already worked on this issue, and encountered the classification of prostheses. Then the information below will be partially or completely known to you. However, we will still pay attention to these aspects, since classifications vary, and in relation to the correct age for installing a prosthesis, it is important for us to understand what kind of prosthesis we are talking about.
Prostheses can be divided depending on the level of amputation or developmental features. For example, upper limb prostheses at the level of the hand and fingers ( hand prosthesis), forearm prostheses, shoulder prosthesis and prostheses after shoulder disarticulation (that is, if the shoulder joint is missing and has to be formed separately).
It is important to understand that this classification is not an absolute guide to action. For example, if your baby has no fingers but a palm, this does not necessarily mean that the kid needs a hand prosthesis. If this palm is immobile, that is, the wrist joint is not formed or is malformed, the hand prosthesis may not fit, the child will not be able to control it. Understanding all the details of this example is not important now, since each hand is individual. This is why it is important to approach the selection of a prosthesis carefully and use the knowledge of specialists in different fields. Thus, in the process of preparation for prosthetics at Motorica, a whole interdisciplinary team of doctors, engineers and prosthetists participates.
Prostheses can be divided depending on the level of amputation or developmental features. For example, upper limb prostheses at the level of the hand and fingers ( hand prosthesis), forearm prostheses, shoulder prosthesis and prostheses after shoulder disarticulation (that is, if the shoulder joint is missing and has to be formed separately).
It is important to understand that this classification is not an absolute guide to action. For example, if your baby has no fingers but a palm, this does not necessarily mean that the kid needs a hand prosthesis. If this palm is immobile, that is, the wrist joint is not formed or is malformed, the hand prosthesis may not fit, the child will not be able to control it. Understanding all the details of this example is not important now, since each hand is individual. This is why it is important to approach the selection of a prosthesis carefully and use the knowledge of specialists in different fields. Thus, in the process of preparation for prosthetics at Motorica, a whole interdisciplinary team of doctors, engineers and prosthetists participates.
Functional classification
Classification by the prosthesis capabilities is the most interesting and important for us. From a functional point of view, prostheses can be divided into three groups:
- cosmetic prostheses;
- active prostheses;
- working prostheses.
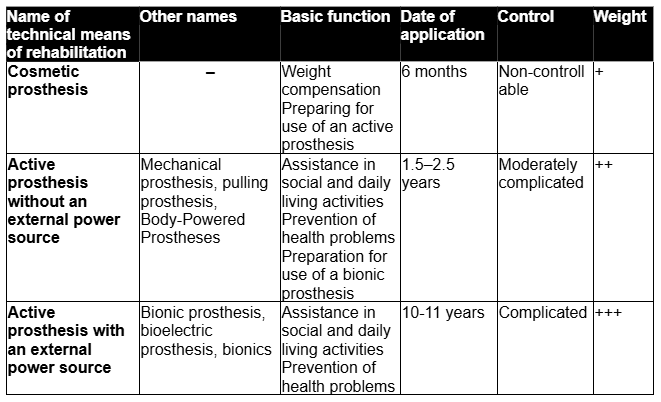
A cosmetic prosthesis is a kind of analogue of a human hand, which is as similar as possible in appearance. There are now prostheses that differ only slightly in their external characteristics from the second limb, you can achieve a similar skin tone, nail shape and even hair. But there will still be differences. At least the artificial hand is absolutely motionless. The cosmetic prosthesis is not capable of performing active movements, meaning it is impossible to pick up objects with it.
Active prostheses, on the contrary, assume the presence of active movements; such devices can be used to pick up objects. Motorica makes such functional prostheses. How the grip occurs depends on the method of controlling the prosthesis, there may be different options.
The first option is when the prosthesis has no external power source. For example, the functional prosthesis of the hand and fingers Kibi or the active prosthesis of the forearm Kibi. The prosthesis moves owing to movements of the arm. The simplest mechanism for controlling the device is is a draw string. For example, the child bends the elbow or wrist, and at this time the links begin to move, flexing the prosthesis fingers. Such devices are also called mechanical or pulling.
The second option is a prosthesis with an external power source. Bionic prosthesis Indy and Manifesto. In this case, the prosthesis has a motor that activates the prosthesis. The task of the person using the device is to give the correct command so that the prosthesis “knows” what action to perform. The most common method of “commanding” a prosthesis is bioelectric. User tenses a certain muscle, sensors read this tension and command the motor to “flex the fingers.” For the fingers to extend, you need to give a new command, for example, tense another muscle. Such prostheses are also called bioelectric or bionic. Surely, bionic prostheses offer more opportunities and have more functions. They can hold heavier items. In addition, in some devices the grasp can be adjusted differently — that is, fingers can be moved separately. However, it is important to understand that bionic prostheses are much more difficult to control. One muscle or another needs to be tensed while completely relaxing the others, and this is not an easy skill. Furthermore, because of the presence of additional elements, such prostheses are significantly heavier than active prostheses without an external power source.
It should be noted separately that in some cases installation of a bionic prosthesis is impossible, as the muscles are atrophied (have lost their strength due to forced inactivity), and the signal from them is insufficient to control the prosthesis. That is why it is so important to get the first prosthesis on time!
A separate chapter can be written about the appearance of Motorica active prostheses — because these devices are created based on the child's design. The kid chooses the color, pattern and attachments themself. And this is an Aladdin's lamp in the process of getting used to a new hand: a bright and unusual prosthesis is perceived as a toy, as something new and very interesting. It is no longer a "torn off hand of a doll", as our kids say about cosmetic devices. The technical means of rehabilitation turn into a robotic arm or a “magic hand”, this is already a sign of superpowers, and it often even causes envy in other children. We had twins undergoing prosthetics, two boys, and only one of them had a special hand. And how much the brother cried when it turned out that the Spider-Man hand was not intended for him, and how proud the happy owner of the prosthesis was. The hardest part, of course, was for their mother – she had to look for a special glove, similar to a prosthesis, so that no one would be offended.
Active prostheses, on the contrary, assume the presence of active movements; such devices can be used to pick up objects. Motorica makes such functional prostheses. How the grip occurs depends on the method of controlling the prosthesis, there may be different options.
The first option is when the prosthesis has no external power source. For example, the functional prosthesis of the hand and fingers Kibi or the active prosthesis of the forearm Kibi. The prosthesis moves owing to movements of the arm. The simplest mechanism for controlling the device is is a draw string. For example, the child bends the elbow or wrist, and at this time the links begin to move, flexing the prosthesis fingers. Such devices are also called mechanical or pulling.
The second option is a prosthesis with an external power source. Bionic prosthesis Indy and Manifesto. In this case, the prosthesis has a motor that activates the prosthesis. The task of the person using the device is to give the correct command so that the prosthesis “knows” what action to perform. The most common method of “commanding” a prosthesis is bioelectric. User tenses a certain muscle, sensors read this tension and command the motor to “flex the fingers.” For the fingers to extend, you need to give a new command, for example, tense another muscle. Such prostheses are also called bioelectric or bionic. Surely, bionic prostheses offer more opportunities and have more functions. They can hold heavier items. In addition, in some devices the grasp can be adjusted differently — that is, fingers can be moved separately. However, it is important to understand that bionic prostheses are much more difficult to control. One muscle or another needs to be tensed while completely relaxing the others, and this is not an easy skill. Furthermore, because of the presence of additional elements, such prostheses are significantly heavier than active prostheses without an external power source.
It should be noted separately that in some cases installation of a bionic prosthesis is impossible, as the muscles are atrophied (have lost their strength due to forced inactivity), and the signal from them is insufficient to control the prosthesis. That is why it is so important to get the first prosthesis on time!
A separate chapter can be written about the appearance of Motorica active prostheses — because these devices are created based on the child's design. The kid chooses the color, pattern and attachments themself. And this is an Aladdin's lamp in the process of getting used to a new hand: a bright and unusual prosthesis is perceived as a toy, as something new and very interesting. It is no longer a "torn off hand of a doll", as our kids say about cosmetic devices. The technical means of rehabilitation turn into a robotic arm or a “magic hand”, this is already a sign of superpowers, and it often even causes envy in other children. We had twins undergoing prosthetics, two boys, and only one of them had a special hand. And how much the brother cried when it turned out that the Spider-Man hand was not intended for him, and how proud the happy owner of the prosthesis was. The hardest part, of course, was for their mother – she had to look for a special glove, similar to a prosthesis, so that no one would be offended.
It is very important not to try to create an analogue of the second hand; the child's prosthesis should be bright and unlike a living hand, because this is how we make it clear that there is no need to be shy and hide the hand.
Finally, let’s discuss the working prostheses. They require the availability of special attachments to perform certain functions. For example, for hammering or sewing. For children, such prostheses are not very relevant. Therefore, we will not go into too much detail about their features - most likely, when your child grows up to them, progress will once again take a step forward, and the information may become outdated. Thus, globally, prostheses can be divided depending on the functions they perform — cosmetic (an attempt to create the appearance of having a hand) or active (a prosthesis with the ability to move and grasp).
At what age should a prosthesis be installed?
It would be more correct to say which prosthesis to install at what age. Because, in essence, all types of prosthesis for a child are relevant and important, but at different periods of life.
According to international recommendations, the first prosthesis should be installed at the age of six months. At this age, a cosmetic prosthesis is installed. Its main purpose is NOT to "disguise" a specific hand. After all, as we wrote above, a child’s hand is beautiful, and there is absolutely no reason to hide it. The main goal of cosmetic prosthetics at this age is to compensate for the weight deficit and equalize the weight of both sides of the body.
Why is prosthetics recommended at six months? Because at about this age the child begins to sit up, and this is a task that requires balance, and it is necessary to “catch” this balance with relatively equal weight of the arms.
Next, the baby masters new motor functions — crawl, stands up, begins to walk — and the kid also needs an even load on both sides of the body. It is important to understand: the more part of the arm is missing, the greater need for a cosmetic prosthesis from a very early age.
A cosmetic prosthesis, when received at six months, has another important task, it forms the habit of wearing a certain device on the hand. Thus, over time, it will not be so difficult for the child to adapt to an active prosthesis. It will be necessary to exchange one prosthesis for another, but not start the process of forming a habit from scratch.
The transition to an active prosthesis occurs at the age of 1.5–2.5 years. The age range is quite wide.
According to international recommendations, the first prosthesis should be installed at the age of six months. At this age, a cosmetic prosthesis is installed. Its main purpose is NOT to "disguise" a specific hand. After all, as we wrote above, a child’s hand is beautiful, and there is absolutely no reason to hide it. The main goal of cosmetic prosthetics at this age is to compensate for the weight deficit and equalize the weight of both sides of the body.
Why is prosthetics recommended at six months? Because at about this age the child begins to sit up, and this is a task that requires balance, and it is necessary to “catch” this balance with relatively equal weight of the arms.
Next, the baby masters new motor functions — crawl, stands up, begins to walk — and the kid also needs an even load on both sides of the body. It is important to understand: the more part of the arm is missing, the greater need for a cosmetic prosthesis from a very early age.
A cosmetic prosthesis, when received at six months, has another important task, it forms the habit of wearing a certain device on the hand. Thus, over time, it will not be so difficult for the child to adapt to an active prosthesis. It will be necessary to exchange one prosthesis for another, but not start the process of forming a habit from scratch.
The transition to an active prosthesis occurs at the age of 1.5–2.5 years. The age range is quite wide.
How do you know if your child is ready for an active prosthesis?
Medical experts, prosthetic developers, prosthetists and parents themselves cite different criteria for readiness. As an example, we will describe here the recommendations of American scientists.
“When a child reaches the age of two, it is necessary to pay attention to the degree of readiness for using an active prosthesis. We do not recommend relying on exact age, as this parameter can be misleading. When making a decision, it is better to rely on compliance with certain criteria:
As can be understood from the abundance of special medical terms, these criteria were developed by doctors for doctors. Therefore, it can be difficult for a parent to assess a child’s readiness at home. We recommend rely on the first four points and, if you have any doubts or questions, seek advice from Motorica. In addition, it is better to start getting used to the prosthesis before the three-year crisis, when the child’s favorite word becomes “no”. The crisis is conventionally given the number 3 in its name, since, according to psychologists, it can occur between the ages of 2.5 and 3.5 years.
Remember, earlier is always better than later! It is important to understand that after all criteria have been met, some time will be required to process the documents, make the prosthesis, and so on. Therefore, the process itself should be started a little earlier.
The type of the first active prosthesis can be any. Today, young children most often use prostheses without an external power source. Motorica bionic prostheses (prostheses with an external power source) are available from 8–11 years old. It's not that a child can't learn to operate a more complex prosthesis. There are known cases where two-year-old children successfully coped with bionic prostheses. But it is important to understand that the cost of these prostheses is significantly higher due to the more complex technical component; the child grows quickly – the prosthesis needs to be changed every year, so the rationality of such expenses remains at the discretion of parents. Such a prosthesis weighs more, and we do not recommend suddenly applying such a load.
What to do with a cosmetic prosthesis after the child has received an active one?
The choice is yours. There are families that continue to use a cosmetic prosthesis, and the child wears it equally with an active one. But most parents prefer to gradually transition to an active prosthesis. And this choice is most often motivated by the fact that an active prosthesis not only compensates for the weight difference between two arms, but also puts a load on the muscles and joints, ensuring grasp. Thus, from a medical point of view, active prostheses have a more pronounced positive effect on the body.
Another important factor is the main message that we want to convey to the child with this or that prosthesis. By maintaining the use of a cosmetic prosthesis at a conscious age, we give the child a clear message - the hand must be hidden, masked so that the feature is not noticeable. But this is not exactly what we want for our child, is it? There is no need to hide arm with or without a prosthesis. There is a peculiarity, and there will also be increased attention from people. And it is better to learn reacting correctly to this attention and accept yourself, regardless of the number of fingers on hands.
It is rare, but it happens that tutors ask not to wear a prosthesis in kindergarten. Most often, they are afraid that they will have to bear responsibility for a breakdown. It is worth immediately explaining or even offering to document the fact that responsibility for the breakdown of prosthesis will not be placed on the kindergarten staff. It is also possible to gently remind that the prosthesis is a technical means of rehabilitation prescribed by a doctor and it is necessary for the child’s health. A decision not to use it can only be made with the consent of the consulting physician.
Comparative characteristics of different types of children's prostheses
“When a child reaches the age of two, it is necessary to pay attention to the degree of readiness for using an active prosthesis. We do not recommend relying on exact age, as this parameter can be misleading. When making a decision, it is better to rely on compliance with certain criteria:
- the child has relatively stable attention and can work on one "task" for about 10 minutes;
- the child is able to follow a two-stage command;
- the child is interested in actions with both hands;
- the child is ready to interact with the prosthetist/rehabilitation specialist;
- the child roughly understands how the prosthesis works and, when interacting with him, realizes that something can be put into his palm;
- the child has a sufficient level of neuromuscular and cognitive development to perform controlled movements."
As can be understood from the abundance of special medical terms, these criteria were developed by doctors for doctors. Therefore, it can be difficult for a parent to assess a child’s readiness at home. We recommend rely on the first four points and, if you have any doubts or questions, seek advice from Motorica. In addition, it is better to start getting used to the prosthesis before the three-year crisis, when the child’s favorite word becomes “no”. The crisis is conventionally given the number 3 in its name, since, according to psychologists, it can occur between the ages of 2.5 and 3.5 years.
Remember, earlier is always better than later! It is important to understand that after all criteria have been met, some time will be required to process the documents, make the prosthesis, and so on. Therefore, the process itself should be started a little earlier.
The type of the first active prosthesis can be any. Today, young children most often use prostheses without an external power source. Motorica bionic prostheses (prostheses with an external power source) are available from 8–11 years old. It's not that a child can't learn to operate a more complex prosthesis. There are known cases where two-year-old children successfully coped with bionic prostheses. But it is important to understand that the cost of these prostheses is significantly higher due to the more complex technical component; the child grows quickly – the prosthesis needs to be changed every year, so the rationality of such expenses remains at the discretion of parents. Such a prosthesis weighs more, and we do not recommend suddenly applying such a load.
What to do with a cosmetic prosthesis after the child has received an active one?
The choice is yours. There are families that continue to use a cosmetic prosthesis, and the child wears it equally with an active one. But most parents prefer to gradually transition to an active prosthesis. And this choice is most often motivated by the fact that an active prosthesis not only compensates for the weight difference between two arms, but also puts a load on the muscles and joints, ensuring grasp. Thus, from a medical point of view, active prostheses have a more pronounced positive effect on the body.
Another important factor is the main message that we want to convey to the child with this or that prosthesis. By maintaining the use of a cosmetic prosthesis at a conscious age, we give the child a clear message - the hand must be hidden, masked so that the feature is not noticeable. But this is not exactly what we want for our child, is it? There is no need to hide arm with or without a prosthesis. There is a peculiarity, and there will also be increased attention from people. And it is better to learn reacting correctly to this attention and accept yourself, regardless of the number of fingers on hands.
It is rare, but it happens that tutors ask not to wear a prosthesis in kindergarten. Most often, they are afraid that they will have to bear responsibility for a breakdown. It is worth immediately explaining or even offering to document the fact that responsibility for the breakdown of prosthesis will not be placed on the kindergarten staff. It is also possible to gently remind that the prosthesis is a technical means of rehabilitation prescribed by a doctor and it is necessary for the child’s health. A decision not to use it can only be made with the consent of the consulting physician.
Comparative characteristics of different types of children's prostheses